Dr. Chet is warmly greeted by a Pokhara VIP.

The Western Regional Hospital(WRH) in Pokhara.

The hallways and clinics at WRH were bustling.

WRH wards were full with patients and their families.

WRH orthopedic patients are admitted for traction.

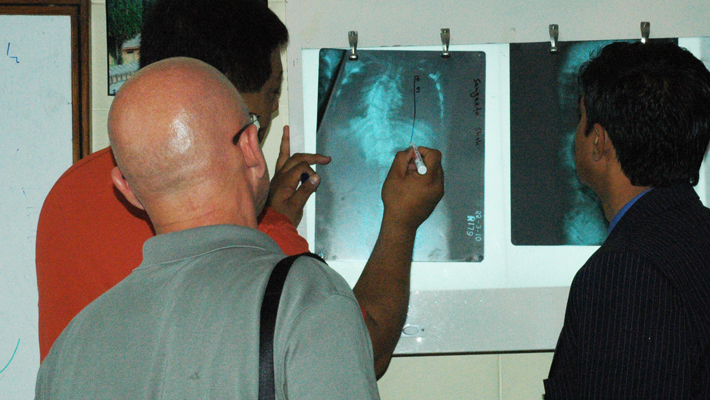
In Kathmandu, I again had the opportunity to operate at the National Trauma Centre (NTS) with professor Giri of the orthopedic faculty at Bir Hospital. A 50 year old female spinal cord injury (SCI). The lateral x-ray revealed a compression injury resulting in an L1 burst fracture with the mild kyphosis.

AP x-ray demonstrated burst fracture of L1 with widened interpedicular distance indicating concomitant lamina fracture.



CT scan sagittal reconstruction demonstrated retro pulsed bone fragment with canal compromise.

CT section confirmed 80-90 degree Celcius canal compromise and lamina fracture.

The patient was placed prone on the OR table with bolsters beneath upper chest and pelvis to assist reduction.

Decompressive Laminectomy was performed with reduction of the retro pulsed bone fragment by direct impact with an angled tamp. Care was taken to minimize manipulation of the conus medullar is. Pedicle screws were placed two levels above and below the burst fracture to compensate for lack of anterior column support after reduction and stabilization. No crosslink's were available, so crossed wire tension band added modest rotational stability. There implants were donated to Spinal Health International by Life Healthcare Pvt. Ltd, N. Ryde (Sydney) NSW, Australia.

However, Nepalis are resilient and resourceful.